Recent articles from two separate research groups published in Scienceand Nature Medicinereport major breakthroughs in flu vaccine research. The advances could ultimately lead to the holy grail of influenza prevention–a universal flu vaccine.
By conferring immunity against large numbers of flu strains, the new vaccines have the potential to reduce the severity of seasonal flu outbreaks and vastly reduce the risk of novel pandemics. Using the RMS Infectious Disease Model, we calculated that if such vaccines were able to confer immunity to 50% of people globally, the risk of a novel flu pandemic outbreak could be reduced by as much as 75%.
This would be a huge success in reducing the risk of excess mortality events and improving global health. Though I should emphasise that while Edward Jenner invented the smallpox vaccine in 1796, it took until 1980 for smallpox to be eradicated from the wild. Beyond development of effective broad-spectrum vaccines, there is a lot of work to do to make the world safe from flu.
A high proportion of flu victims are the elderly. Significantly reducing deaths from flu would disproportionately reduce old-age mortality. This is particularly interesting; not only is it an important milestone in improving old-age public health, it is also relevant to old-age care and budgeting for retirement too.
Influenza Is The Most Likely Source of Future Pandemic Sickness and Mortality.
In the U.S., in a single flu season, the average number of flu-related deaths is 30-40,000, peaking at 47,000 deaths in previous seasons. This does not take account of the viruses that can cause major pandemics: death tolls in the 1918 “Spanish Flu” event reached as high 50-100 million people worldwide.
Widespread use of a universal vaccine conferring lifelong immunity could eliminate these deaths, making a meaningful contribution to reducing infectious disease mortality.
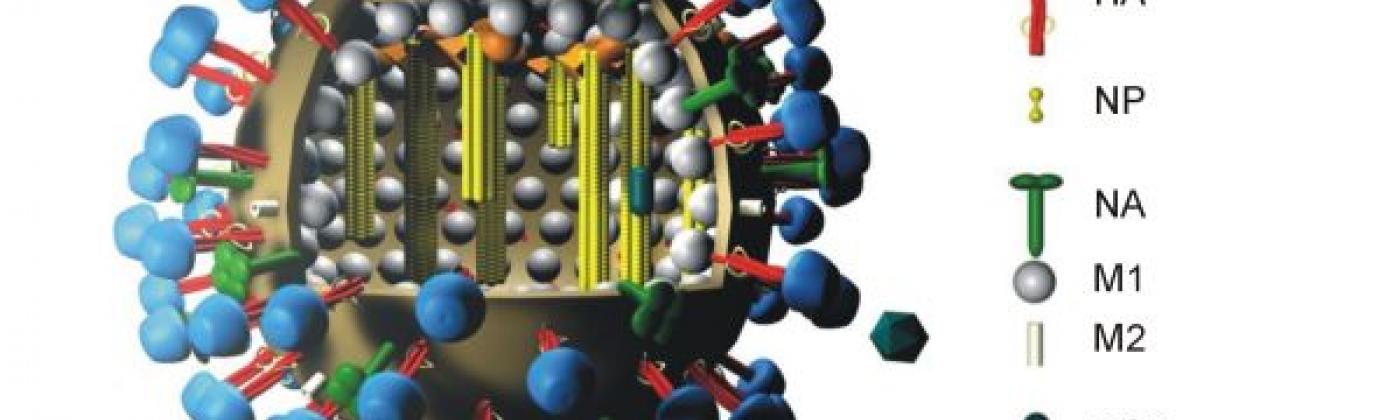
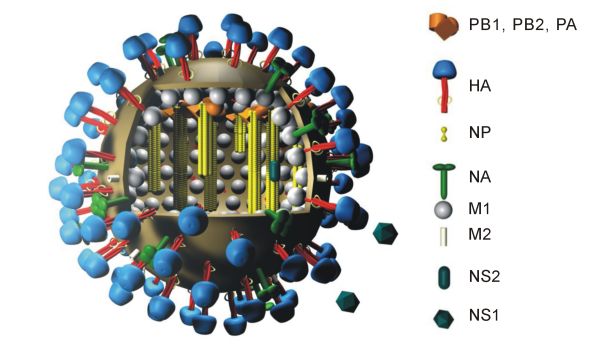
Structure of influenza, showing hemagglutinin as HA. Source
The marvel of the new vaccines under development is their potential to confer immunity against many strains, including ones that have not yet emerged. They work by using cutting-edge molecular machinery to target the stem of the haemagglutinin protein on the virus’ surface. The vaccines have only been tested on animal models and only on a small scale so far, but have worked well in reducing viral loads and mortality in these tests.
If this breakthrough translates into future vaccines that prove efficacious in clinical trials, these could become immensely powerful in combatting both seasonal flu cases and reducing the likelihood of new flu pandemics.
Today, beyond seasonal flu, there are no vaccines capable of preventing novel flu pandemics. However, the production pipeline for the current seasonal flu vaccine can be put to use in pandemics, with current capacity of pipelines estimated to produce decisive quantities of vaccine within three months of a pandemic outbreak.
As quantified in the RMS Infectious Disease Model, while this current technology has the potential to substantially reduce the total caseload of a pandemic, it is not a panacea. Three months is a relatively long time for highly transmissible viruses, so very large numbers of people could be infected in this interval. Even more infections would happen during the roll-out period before the vaccine has successfully been given to sufficient people to halt the spread. Furthermore, complications could emerge during the production that either mean it takes longer than three months, or that such a vaccine only confers partial immunity.
RMS created the world’s first probabilistic model of pandemic influenza and the first probabilistic model of vaccine development, delivery, and efficacy. The recent breakthroughs in flu vaccine research are welcome news and RMS scientists are closely monitoring the developments.
Share:
You May Also Like
November 03, 2014
Ebola in the U.S. – How big of problem are we looking at?
As mentioned in my previous blog post, Ebola has the potential to be one of the deadliest epidemics in a century, but the primary area of concern is Western Africa, where the virus is most prevalent. However, as cases pop up in the U.S., concerns are rising, as evidenced by the acute media analysis and discussion around the first case in New York, for example.
Based on RMS modeling, we estimate that there will be between 15 and 130 cases in the U.S. between now and the end of the year—less than 1 case for every 2 million people. Our calculations assume that American medical professionals working with infected people in West Africa will account for the majority of cases. We simulated the number of new U.S. cases based on the existing infection rates among the American medical workers; this technique incorporates our projections for future West African caseloads and medical staff on the ground in the next two months, based on RMS’s epidemic scenario model. We then further modeled the virus’s spread once back in the U.S., taking into account the preparedness and higher quality of treatment facilities here versus the affected countries in West Africa.
The high end of the range is likely a slight overestimate as our calculations exclude automatic quarantining measures that some areas of the US are implementing. These measures can both reduce the number of contacts (people who come into contact with the infected person) for the imported cases, as well as increase the travel burden on U.S. volunteers planning to support the effort in Africa; this in turn could potentially reduce the number of people who actually make it over to the affected region.
The U.S. is prepared to handle the caseload even if it hits the upper range of 130 new cases. At any given time between now and December, specialized Ebola biocontainment facilities will have 11 beds available, which is enough to cope with the maximum weekly caseload in most of (but not all) of our modeled projections. In the more extreme scenarios, we still expect hospitals nationwide that have at least one Ebola treatment bed in place to handle overflow. Even if the reality over the next few months resembles a very pessimistic situation, it will be manageable given the U.S.’s higher capacity for managing cases.
Catastrophe modeling is an art and a science. The interesting, albeit challenging, part about calculating a range for something like this is that so much is contingent on estimates. The very nature of the virus and the exponential way the epidemic spreads means our estimates of the uncertainty in the variables are amplified in the number of cases. Our estimate is largely dependent on when affected regions reach the tipping point, where the number of new daily cases declines rather than increases. Everything is interconnected – the pace at which the epidemic spreads directly affects the tipping point, which then affects the need for treatment and number of professionals, which in turn affects the potential number of cases that can be imported back to the U.S.
As with all catastrophes we model, understanding risk is the first step toward mitigating and managing it.…
Ebola is a hot topic in the media right now, with multiple cases being reported outside of West Africa and much confusion among the general public around the reality of the danger. So, are the fear and sensationalism warranted?
RMS models infectious diseases and recently developed the world’s first probabilistic model for the current West African Ebola outbreak. While Ebola is indeed a very scary and relatively deadly disease, with a case fatality rate between 69 and 73 percent according to the WHO, RMS modeling shows that it is unlikely the outbreak will become a significant threat globally.
The spread of Ebola in West Africa is in part due to misconceptions and fear surrounding the disease and a lack of public health practices. Ebola can be passed solely via bodily fluids; the risk of unknowingly contracting the disease is low.
Fear is prevalent among some West African communities that Ebola is a lie or is being used purposefully to wipe out certain ethnic groups, causing them to hide sick family members from healthcare and aid workers. Customary burial practices, in which family members kiss and interact with the dead, also have contributed to Ebola’s spread. Getting the populace in these countries to trust foreigners who are telling them to abandon their customs has been an uphill struggle.
In more developed countries where health care is more advanced and understood, the chances of transmission are exponentially smaller due to the fact that extreme containment measures are taken. Controlling the spread of the disease comes down to a question of logistics; if the medical community can control the existing cases and trace the contact made with carriers, spread is much less likely. For example, the case in Texas can be contained to one degree as long as every single person in contact with the patient is tracked.
There is also a (speculative) fear of the virus mutating into an airborne pathogen; the fact is, the chances of the virus changing the way it is transmitted, from fluid contact to airborne passage, are very low and of a similar order of magnitude to the chance of emergence of a different highly virulent novel pathogen.
Vincent Racaniello, a prominent virologist at Columbia University wrote:
“When it comes to viruses, it is always difficult to predict what they can or cannot do. It is instructive, however, to see what viruses have done in the past, and use that information to guide our thinking. Therefore, we can ask: has any human virus ever changed its mode of transmission? The answer is no. We have been studying viruses for over 100 years, and we’ve never seen a human virus change the way it is transmitted.”
The tipping point in the modeling of a virus like Ebola is the point where the resources being used to mitigate the threat outpace the increase in new cases. Trying to get ahead of the epidemic itself is like a race against a moving target, but as long as people get into treatment centers, progress will be made in getting ahead of the illness.
So, while Ebola is a very scary and dangerous illness, it is not something that we expect to become a global pandemic. However, while the current outbreak is not expected to spread significantly beyond West Africa, it still has the potential to be the most deadly infectious disease in a century and could have drastic economic impacts on the communities that suffer from Ebola breakouts. In fact, the economic impacts are likely to be worse than the actual impacts of the disease, due to negative impacts to trade and inter-community relations.
The key is to contain it where it is, reach the tipping point as quickly as possible, and to promote safety around existing infected persons. Through travel control measures and the development of several new drugs to combat the virus, the danger of epidemic should be drastically reduced in Africa and, as a result, the rest of the world.…
Dominic is the head of consulting in the LifeRisks team at RMS. He leads medical modeling projects related to longevity risk, mortality-longevity hedging, excess mortality and morbidity for clients in the (re)insurance and pensions sectors, and the broader field of catastrophe risk reduction. Dominic has modeled several live disease events, including the 2009 H1N1 Swine Flu pandemic and the 2014 West African Ebola outbreak. Dominic also leads RMS' work on structuring and modeling transactions that protect organizations against the financial impact of mortality events. Dominic guided the RMS analytics team through the groundbreaking Vita Capital IV transaction in 2009, the first transaction designed to cover an ongoing influenza pandemic, and the Kortis Capital and Catherine longevity trend risk transactions. Dominic holds an MA in Natural Sciences from the University of Cambridge and an MSc in Systems Biology from Imperial College London, and is a CFA Charterholder.



#/media/File:Flu_und_legende_color_c.jpg){kind=link}